
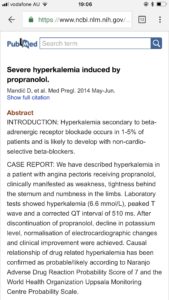
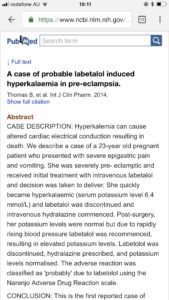
Podcast: Play in new window | Download (Duration: 19:07 — 17.5MB)
Subscribe: Apple Podcasts | RSS | More
Merry Xmas!
This weeks post was inspired by a recent unexpected case of severe hyperkalaemia in a severe pre-eclamptic – I have put together a fictitious case which is a little more severe in order to illustrate the principles of managing hyperkalaemia – I hope you enjoy & take it easy over Xmas!
CASE HISTORY
(*A fictitious patient history )
Your pager goes off – code blue medical labour ward! On arrival you are told the patient for whom the code was called has just arrived following an urgent transfer from another hospital. She presented to their service at 31 weeks with a headache, BP 190/100, proteinuria and mildly raised creatinine. She was diagnosed with severe pre-eclampsia, given labetalol, nifedipine and then transferred. She now appears confused with the following vital signs:
HR 33/min, BP 74/55, SpO2 92%, RR 17/min

(*Image courtesy www.lifeinthefastlane )
{kind=link}
An immediate venous blood gas shows the following result:
Na 139, K 8.4, pH 7.23, pCO2 37, pO2 63, Lactate 1.8
How are you going to manage this patient?
Immediate Standard Mgmt
1 – Is it real?
Common causes of high potassium includes hemolysis of red cells from the sampling and handling process. Always do an ECG whilst awaiting a repeat result – if the patient is compromised and the ECG is abnormal / consistent with hyperkalaemia then assume it is real and don’t delay your treatment! The quickest way to get a repeat sample is usually a VBG this usually only takes a few minutes and will also give you the glucose and pH – important values to know for both mgmt and diagnosis.
2 – Prevent an arrhthymia
Immediate mgmt – stabilise the cardiac membrane with intravenous calcium. Most guidelines recommend calcium if there are ECG changes or the absolute K level is over 7mmol/L.
*Calcium chloride has 3 times more calcium than calcium gluconate.
3 – Shift K intracellularly
a) Insulin / Glucose. Usual dose 10units actrapid + 25-50ml 50% Dextrose
- Stimulates Na/K/ATPase
- Give glucose to prevent hypoglycaemia’
- Lowers K by 0.5 -1 mmol/L per hour
b) Salbutamol
- 20mg neb
- Good choice if the patient is bradycardic (common in severe hyperK)
- Stimulates Na/K/ATPase also
c) NaHCO3 (if acidotic)
- When acidosis exists H+ is exchanged for intracellular K+
- Makes sense to consider NaHCO3 if acidosis is present
- 50-100ml of NaHCO3 8.4%
4 – Eliminate K from the body (usually renal)
– Enhance renal elimination – diuretics (e.g. frusemide), K free crystalloid (if indicated – saline) or both!
– Dialysis – institute early in patients with complete renal failure
– GI exchange resins (eg resonium) most guidelines now consider they have no role in the acute management.
5 – Identify and treat the cause! – You need to address this issue to stop if from recurring!
- Usually multiple factors combine to lead to hyperkalaemia.
- Fix reversible causes especially drugs! Don’t rely on your memory – get their medication chart out then google all the known drugs that can cause hyperkalaemia!
- Drugs Known to Cause / Contribute to hyperkalaemia (either impair excretion or promote transcellular shift)
- ACE inhibitors / AT2 antagonists
- Spironolactone / Amiloride
- NSAIDs
- Beta blockers (see discussion below)
- Trimethoprim
- Heparin
- Pentamidine
- Suxamethonium
- Renal dysfunction – almost always there is a degree of renal impairment preventing excretion of the excess K load. Make sure you aren’t missing important reversible causes – e.g. obstruction (consider USS renal tract urgently).
- Cell release (eg hemolysis, tumour lysis, trauma or extensive surgical injury). In our O& G patients this includes widespread tissue injury especially after major surgery or perhaps chemotherapy.
BUT
- This is a pregnant woman with PET – renal impairment, acidosis, hemolysis, transfusion – these are common events in our pregnant patients.
Cardiac Arrest Secondary to Hyperkalaemia
Adrenaline (beta agonist) – will move K into cells, NaHCO3, Calcium and more calcium!
Important principle: Never stop resuscitation until the potassium is normalised (much like in hypothermic arrest – they are not dead until they are warm and dead!)
There are successful case reports of dialysis or ECMO being used during refractory arrest with good neurological outcomes.
Hyperkalaemia and PET
1 – Beware: Intravenous Ca is a mild vasoconstrictor and can worsen the hypertension transiently – this is what we observed in a recent case I was involved in.
2 – Beta blockers can contribute to / cause hyperkalaemia (the same mechanism but opposite effect of the use of salbutamol / beta2 agonists ) – labetalol is commonly used in these patients – consider changing to another antihypertensive like hydralazine and/or diuretics if the patient remains severely hypertensive (note loop diuretics will also help excrete K!)
3 – Nifedipine is a ca antagonist (altho less cardiac specific) – does this have implications for the effectiveness of Ca? Will these increase the toxicity of the hyperkalaemia?
4 – Diuretics – these are ok in PET and pregnancy as long as there is a good indication – severe hyperkalaemia (and hypertension) is!
What are the ECG changes you see with hyperkalaemia?
Links / References:
Great Podcasts:
https://emcrit.org/emcrit/hyperkalemia/
LITFL management principles:
Causes of hyperkalaemia:
Precious Bodily Fluids – the musings of a salt whisperer.
Possibly the best website / resource for electrolytes anywhere – full stop. Check out their free 500+ page textbook here:
http://pbfluids.com/the-electrolyte-book/
Remember, hyperkalaemia is the syphilis of the ECG world – it can be a very sneaky mimic!
Drugs Known to Cause / Contribute to hyperkalaemia
Great description here on LITFL: